3.1 INTRODUCTION
Diagnostic coding has a long history of development. The first edition, which originated in the year 1850, was actually known as the ‘International List of Causes of Death. The International Statistical Institute adopted this first edition in 1893 and the World Health Organization (WHO) took over responsibility for the ICD from 1948 when the WHO had its beginnings. By that time the ICD was in its Sixth Revision, which for the first time included causes of morbidity. [1]
In 1967 The World Health Assembly adopted the WHO Nomenclature Regulations that stipulate use of the ICD in its most current revision, for mortality and morbidity statistics by all Member States. [2]
The WHO ‘International Statistical Classification of Diseases and Related Health Problems’ now in its 10th Revision is available ‘Online’ and is an extensive document covering 22 Chapters in its Version for 2010. [3]
3.2 INTERNATIONAL CLASSIFICATION OF DISEASES (ICD)
In explanation of what the ICD embraces the following information, provided by the WHO, is both succinct and informative as to how and why the codes are used [4]:
The ICD is the international standard diagnostic classification for all general epidemiological, many health management purposes and clinical use. These include the analysis of the general health situation of population groups and monitoring of the incidence and prevalence of diseases and other health problems in relation to other variables such as the characteristics and circumstances of the individuals affected, reimbursement, resource allocation, quality and guidelines.
‘It is used to classify diseases and other health problems recorded on many types of health and vital records including death certificates and health records. In addition to enabling the storage and retrieval of diagnostic information for clinical, epidemiological and quality purposes, these records also provide the basis for the compilation of national mortality and morbidity statistics by WHO Member States.’
Current information, with quite regular updates, relating to what has come to be known as ’The WHO Family of International Classifications’ is readily accessible online, and does not warrant reproduction here.What should be noted however, are the links to a very valuable 27 page document titled ’World Health Organisation Family of International Classifications: definition, scope and purpose.’ [5]
This document, which has evolved from earlier work by the same authors, presents clear pictures of the various elements which make up the WHO family of classifications.
Its authors, Richard Madden of the National Centre for Classification in Health, Australia, Catherine Sykes of the Australian Institute of Health and Welfare and T Bedirhan Ustun of the World Health Organization give due acknowledgement of earlier input from Dr John Ashley (United Kingdom) and Dr Willem Hirs (Netherlands) and many members of the WHO-FIC Family Development Committee and Planning Committee over a seven year period (2000-2007). They also acknowledge the contribution from Ms Marjorie Greenberg of the United States. [5]
The following detail given in Figure 1 of this dissertation gives a clear picture of how elements of the “WHO family” inter-relate [5]:
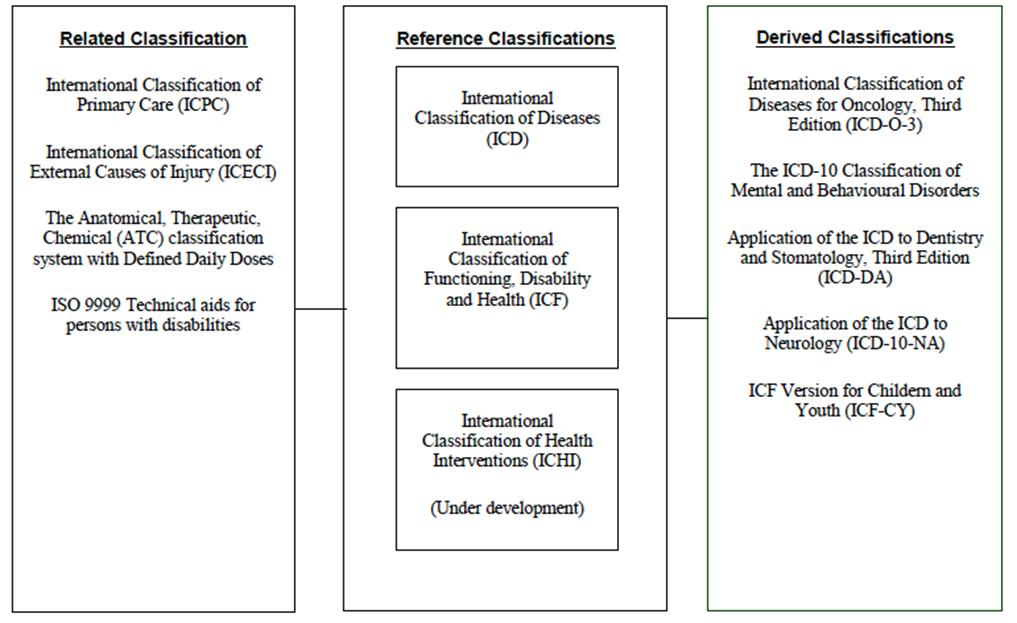
Figure 1: Schematic Representation of the WHO-FIC
An announcement made on the 22nd July 2010 is quite pertinent to the effective utilization of the various codes. The WHO and the International Health Terminology Standard Development Organisation (IHTSDO) have collaborated to link the terminologies and classifications of the WHO Family of Classifications and the Standardized Nomenclature of Medicine – Clinical Terms (SNOMED CT). It is seen as a major step forward in this era of electronic health records and information. [4]
The actual announcement of what is termed ’the harmonization’ was carried in the following letter [5]:
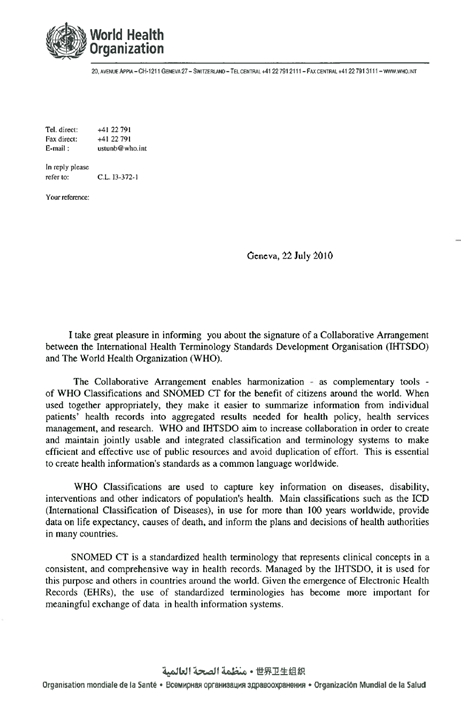
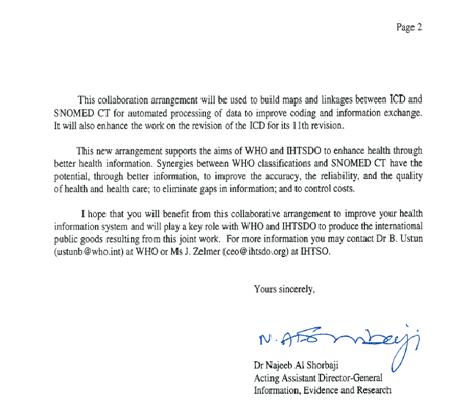
Figure 2: Letter of Collaborative Arrangement between the International Health Terminology Standards Development Organisation (IHTSDO) and The World Health Organization (WHO)
Specific Coding for Chiropractic
In the United States of America the chiropractic profession has the responsibility of submitting accurate coding for all procedures utilized in caring for patients when such care is billed to Medicare or other third party payers. A Coding and payment Guide for Chiropractic Services has been made available and this document is updated from year to year as deemed necessary. [6]
1. Coding and Payment Guide for Chiropractic Services: 2010 Edition
This coding guide helps assist chiropractors in dealing with coding, documentation and reimbursement issues. Extracts from the Fifth Edition 2008 document are displayed in Appendix 1 giving an indication, through its index, of the size of such a guide which consists of 372 pages. [7] The latest coding and payment guide for 2013 will be available from Dec 2012. [8]
2. Commonly Used ICD-9 Codes in Chiropractic offices.
The Diagnosis Codes (ICD-9) that are often used in chiropractic centres have been discusses and outlined by Dr Frank M Painter at the Chiropractic Resource Organization. [9]
Dr. Painter explains how this material is used in a “cover letter” which is forwarded to “insurers, along with the full diagnosis, so they will understand our use of the codes, and what it is we are describing. [9]
In his cover letter he introduces the subluxation and its’ five component parts and which codes each relates to each part. For example Kinesiopathology is covered in codes 739 and 839 and the 737 ICD-9-CM codes. Neuropathology, is addressed under 722-24, 353 ICD-9-CM codes. Myopathology is covered by the 728-29, 847 ICD-9-CM codes. Histopathology, is under the 719, 782 ICD-9-CM codes and Pathophysiology is within the 732-39, 723 ICD-9-CM codes. [9]
We have set out below some of the ICD-9 Codes used by chiropractors based on body region and complaint. [9]
The Cervical Spine:
The MEDICARE listings for Subluxation (the 739 series):
- 739.0 – Occipital Subluxation
- 739.1 – Cervical Subluxation
- 739.2 – Thoracic Subluxation
- 739.3 – Lumbar Subluxation
- 739.4 – Sacroiliac Subluxation
Listing for Subluxation (the 839 series):
- 839.01 – Subluxation of First Cervical Vertebra (Dislocation, closed)
- 839.02 – Subluxation of First Second Vertebra (.03 = Third, etc. etc.)
- 839.08 – Multiple Cervical Subluxation
- 722.0 – Cervical Disc Disorder w/o Myelopathy
- 722.71 – Cervical Disc Disorder with Myelopathy
- 723.0 – Cervical Spinal Stenosis (usually Disc-related)
- 722.4 – Degeneration of Cervical Disc(s)
- 353.2 – Cervical Nerve Root Lesion
- 354.2 – Ulnar Nerve Lesion
- 354.3 – Radial Nerve Lesion
- 719.58 – Stiffness of Cervical Spine
- 847.0 – Cervical Sprain/Strain
- 723.8 – Occipital Neuralgia
- 723.3 – Cervicobrachial Syndrome
- 353.0 – Thoracic Outlet Syndrome
- 726.1 – Rotator Cuff Syndrome
- 726.10 – Supraspinatus Syndrome
- 354.0 – Carpal Tunnel Syndrome
The Thoracic Spine:
- 839.21 – Subluxation of the Thoracic Vertebrae
- 722.51 – Degeneration of Thoracic Disc(s)
- 847.1 – Thoracic Sprain/Strain
- 719.08 – Edema of Thoracic Facet Joint
- 719.48 – Arthralgia of Thoracic Spine
- 719.58 – Stiffness of Thoracic Spine
The Lumbar Spine:
- 839.20 – Subluxation of the Lumbar Vertebrae
- 722.10 – Lumbar Disc Disorder w/o Myelopathy
- 722.73 – Lumbar Disc Disorder with Myelopathy
- 722.52 – Degeneration of Lumbar Disc(s)
- 738.4 – Spondylolysis/Spondylolisthesis (Acquired)
- 756.12 – Spondylolysis (Congenital)
- 724.3 – Sciatica; Neuralgia of Sciatic Nerve
- 724.9 – Foraminal Encroachment (Compression) of Nerve Root, Lumbar
- 353.4 – Lumbosacral Nerve Root Lesion
- 847.2 – Lumbar Sprain/Strain
- 719.48 – Arthralgia of Lumbar Spine
- 719.58 – Stiffness of Lumbar Spine
The Pelvis:
- 839.42 – Subluxation of the Sacroiliac Joint
- 847.3 – Sacroiliac (SI) Sprain/Strain
- 353.1 – Lumbosacral Plexus Lesion
- 720.2 – Sacroilitis
- 839.41 – Subluxation of the Coccyx
- 847.4 – Coccyx Sprain/Strain
- 353.1 – Lumbosacral Plexus Lesion
The Peripheral Joint Codes:
- 831.01 – Anterior Subluxation of Humerus
- 831.02 – Posterior Subluxation of Humerus
- 832.12 – Subluxation of Elbow
- 833.03 – Subluxation of Carpal Bone
- 836.53 – Medial Subluxation of Tibia
- 836.54 – Lateral Subluxation of Tibia
- 838.01 – Subluxation of Tarsal Bone
- 719.06 – Edema of Knee joint/Fibula/Patella/Tibia
- 719.07 – Edema of Ankle/Foot Joints
Sprains and Strains of Shoulder and Upper Arm:
- 840.0 – Acromioclavicular (joint) (ligament)
- 840.6 – Supraspinatus (muscle) (tendon)
Various Other Codes:
- 733.1 – Collapsed Vertebra
- 805.2 – Compression Fracture
- 805.4 – Compression Fracture Lumbar
- 724.9 – Ankylosing Spondylitis (Ankylosis of Spine)
- 781.9 – Abnormal Posture
- 737.10 – Kyphosis (Acquired)
- 737.20 – Lordosis (Acquired)
- 738.2 – Hypolordosis of the Cervical/Lumbar Spine (Acquired)
- 738.2 – Reversal of the Cervical Curve
- 737.30 – Scoliosis (Idiopathic)
- 715.9 – Degenerative Joint Disease (Osteoarthritis)
- 715.95 – Degenerative Joint Disease of the Hip
- 734 – Pes Planus, Acquired
- 754.61 – Pes Planus, Congenital
- 736.41 – Genu Valgus
- 733.0 – Osteoporosis
- 733.01 – Osteoporosis Senile
- 733.02 – Osteoporosis Idiopathic
SYMPTOMS:
- 723.1 – Cervicalgia
- 724.1 – Thoracic Spine Pain
- 724.2 – Lumbalgia
- 648.70 – Pregnancy Backache
- 724.5 – Vertebrogenic Pain Syndrome
- 726.90 – Tendinitis/Capsulitis
- 727.00 – Synovitis/Tenosynovitis
- 727.3 – Bursitis
- 729.1 – Myofascitis of Upper Extremity Musculature
- 729.1 – Myofascitis of Lower Extremity Musculature
- 728.87 – Muscle Weakness
- 728.85 – Muscle Spasm
- 780.4 – Dizziness
- 438.85 – Vertigo
- 787.0 – Nausea
- 782.0 – Paresthesia/Tingling/Burning/Prickling
- 354.8 – Nerve Inflammation/Compression (Upper Limb)
- 443.0 – Raynaud’s Syndrome
- 354.4 – Causalgia of Upper Limb
- 726.0 – Adhesive Capsulitis of Shoulder
- 726.11 – Calcific Tendinitis of Shoulder
- 726.12 – Bicipital Tenosynovitis [9]
3. How to correctly assign the diagnosis code for speedy payment
Within the same publication of The Chiropractic Resource Organization, Dr. Alan L. Lyons from D.C. of California who is highly qualified in this area has presented what has become an essential reference document for chiropractors in the USA involved with any issues relating to the Diagnosis Codes used in Chiropractic practice. His guidelines are designed to assist with faster payment and less review for the practicing chiropractor. [10]
He notes that the proper coding of a diagnosis is very important with accuracy ensuring not only reimbursement but also protection from legal action.
He sets out the following examples:
- 353.0 – brachial plexus compression 353.2 cervical root lesions
- 723.1 – cervicalgia 723.2 cervicocranial syndrome
- 723.3 – cervicobrachial syndrome 723.8 cervical syndrome
- 724.02 – lumbar spinal stenosis 724.5 backache (pain) syndrome
These codes are often used in chiropractic centres and none of them support chiropractic care. These codes are not used when there is a disc problem or spondylosis.
Using the wrong codes repeatedly can lead to malpractice issues and problems with professional registration. For reimbursement the Medicare system in the USA requires the ICD-9-CM and CPT codes to be used.
It is important to understand the difference between signs, symptoms and the definitive diagnosis.
The definitive diagnosis is the cause of the patients actual problem. It provides the justification for treatment and payment for treatment. It is important to note that the definitive diagnosis contains all the signs and symptoms relevant to the diagnosis. Thus, when a definitive diagnosis code is used the signs and symptoms are specifically excluded from the diagnostic coding statement. If the codes for the signs and symptoms are included as well, it will lead to an insurance review and delayed payment.
If you are unable to determine the cause of the patient’s problem then you can use the codes for signs and symptoms. However signs and symptoms are non-specific and don’t provide clinical justification for the use of chiropractic adjustment. A description of a misalignment is needed to justify manipulation. Some examples are subluxation, sprain/strain laxity of ligament.
Terms that are not descriptive of a misalignment and thus don’t support chiropractic manipulation include neuritis and myelopathy. [10]
a) Sample Cases of Correct ICD-9-CM Codes
1. Male complains of low back pain with sciatica following a fall at work today from a ladder. Examination and x-ray findings are a right PI ilium and L5 subluxation with some OA.
This needs to be an acute diagnosis code as it is less than 31 days from the injury date. Possible codes to use are:
- 846.1 – sacroiliac ligament sprain/strain
- 846.0 – lumbosacral sprain/strain (L5-S1)
- E881.0 – fall from a ladder
- E849.3 – place of occurrence, industrial place and premises
The Doctor has the choice to use either sprain/strain or the subluxation codes.
If it was more than 30 days post injury, then the chronic diagnosis codes are used. They are:
- 728.4 – laxity of ligament
- 905.7 – late effects of sprain/strain w/o tendon injury
- E929.3 – late effects of accidental fall
- E881.0 – fall from a ladder
- E849.3 – place of occurrence, industrial place and premises
It is notable that the code 905.7 indicates that 728.4 is the consequence of 846.1 and 846.0 and not a new or unrelated diagnosis. E codes inform the insurer of the details of the original injury. [11]
b) Using the ICD-9-CM Codes – The Diagnosis Codes Must Support the Procedure Codes
A diagnosis needs to be given that supports the need for each treatment that the patient receives.
Some basic guidelines are set out below.
1. ICD-9-CM codes ranging from 001.0 through V82.9 are used to give the diagnosis and reason for the treatment.
- Codes within the range of 001.0 through 999.9 are for disease classification. Symptom based codes are of diseases and injuries. Codes that describe symptoms are only allowable when that is the highest level of diagnosis able to be certainly documented.
- In case of visits for matters unrelated to disease uses the codes V01.0 through to V82.9 are used.
2. Always list the primary diagnosis first. Other codes are place after.
3. Use the most specific ICD-9-CM codes possible. Use the 5 digit codes, then the 4 digit codes and only use the 3 digit codes when there are no 4 digit codes.
4. Unconfirmed diagnoses should not be coded as if they are a confirmed diagnosis.
5. When diagnostic services are the sole reason for a visit. Use the “V code” for the diagnostic procedure (e.g. X-ray) and then list the actual problem code second. If the second code is not listed payment delays can occur.
There are Medicare penalties for non-compliance with coding practices. They include having claims returned and payment being withheld. In certain cases the Doctor may be subject to a civil monetary penalty for refusing to provide the codes. Repeated failure to provide codes by a professional can lead to exclusion from the Medicare program.
For chiropractors using Medicare:
- The service provided is manual manipulation of the spine. The procedure code for this service is A2000.
- Subluxation of the spine must be the primary diagnosis must be, either so stated or identified by a term descriptive of the subluxation.
Acceptable diagnoses include intervertebral disc disorders 722.0-722.9; curvature of the spine 737.0-737.9; spondylolisthesis 738.4-756.12; spondylolysis 756.11. Also the spinal level of the subluxation needs to be included. [10]
c) Down Coding
Down coding is when a code is changed from a higher value to a lower value code. Usually it leads to lower reimbursement.
When there are co-existing conditions which can complicate treatment of the primary problem, the doctors must list the icd-9-cm codes of the coexisting problems as well. This is important to justify treatments given. [10]
The most severe injury is the primary diagnosis, when there are multiple injuries. An appropriate E-Code needs to be used to show the cause of the injury.
Injuries are categorized by type, then divided by anatomical region. The codes in Categories 800-959 cover such injuries as fractures, dislocations, and sprains. [10]
E-Codes Usage
E-codes provide for describing environmental issues as the injury cause. The use of an E-code along with the injury identification code gives extra information relevant to industry, insurance and public health bodies.
E-Codes are not used alone as the principal codes. They must be used in conjunction with the main codes 001-999 to show the cause of the problem E-codes give important accident details of an accident to insurance companies allowing fast and accurate payments.
The E-codes are used secondary to the injury code. For example:
Rib fracture; Occurred at home falling from a ladder.
Codes to use:
- 807.00 – Fracture of ribs, closed, unspecified; (followed by E codes)
- E881.0 – Fall from ladder and E849.0 Place of occurrence, home[10]
d) Using Late Effects Coding
Late effects codes are used after the acute phase of an injury has passed, but a problem still remains, i.e. a residual effect.
In order to code properly, the code for the residual condition is listed first followed by the code for the original illness. There are late effects E Code that can be used as well. Other late effects codes are found in category 905-909 (Miscellaneous). [10]
e) How to Use Acute and Chronic Coding
- When there are separate problems in acute, and chronic, phases then use both codes. Put the acute code first.
- If a certain condition is a sub-acute condition but there is no code for sub-acute, then use the acute code. [10]
f) Codes Commonly used by Chiropractors.
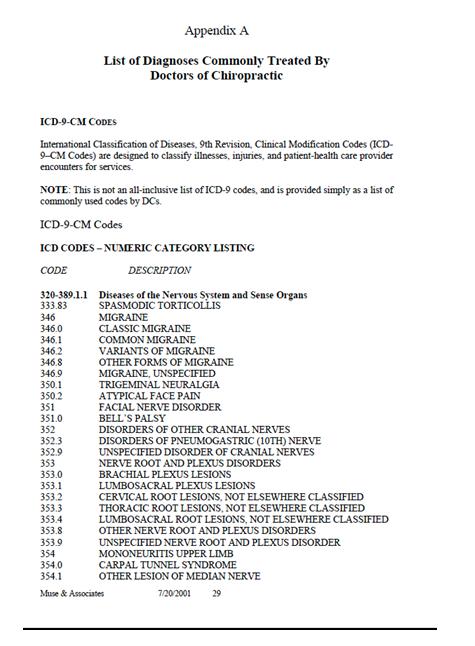
In July of 2001 the American Chiropractic Association published a report on a study conducted by Muse and Associates a private company categorized under Health Care Management and located in Washington, DC. [11]
In their study Muse and Associates had examined Medicare program costs for Chiropractic services. They compared the treatment costs for chiropractic against those of other providers. From the report, Muse and Associates suggest there is some misconception about chiropractors’ only treating low back pain. [12]
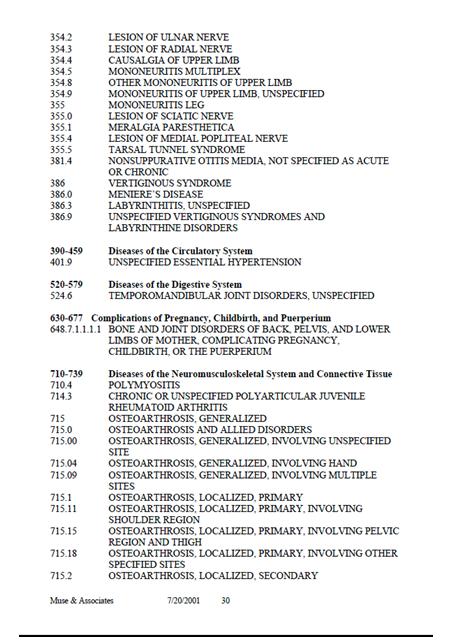
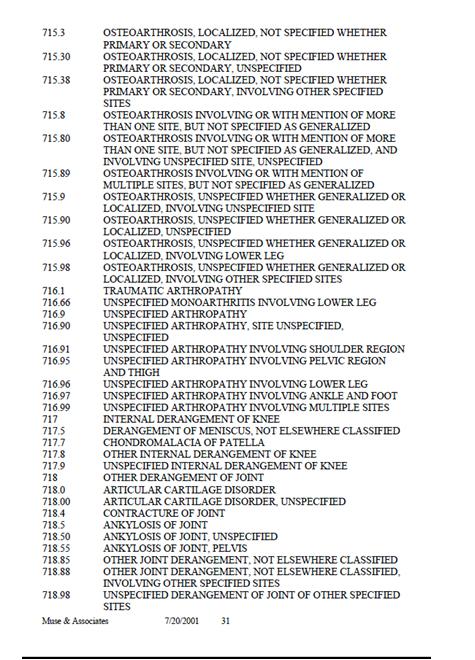
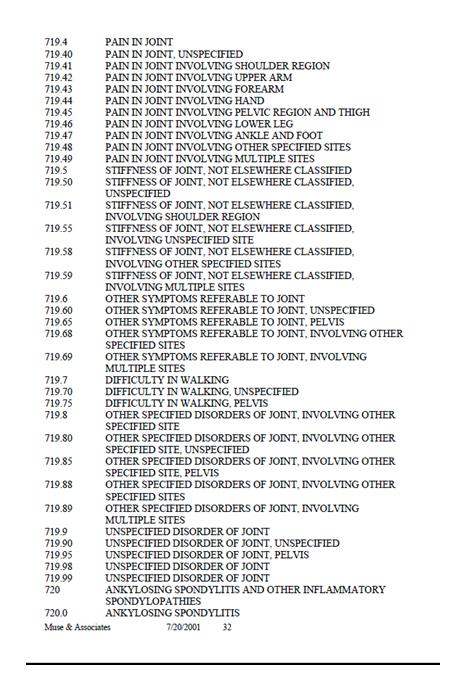
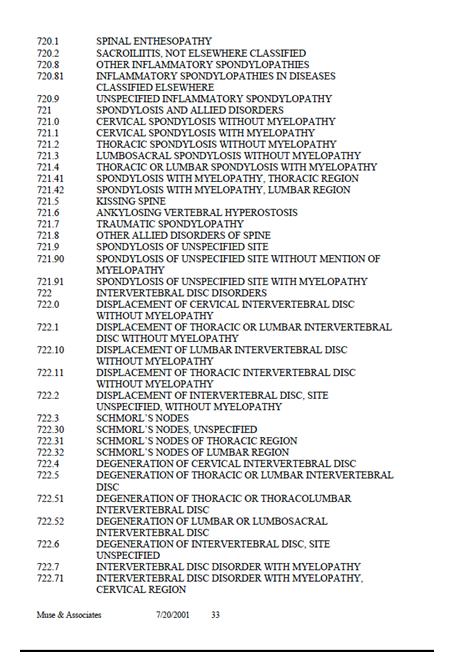
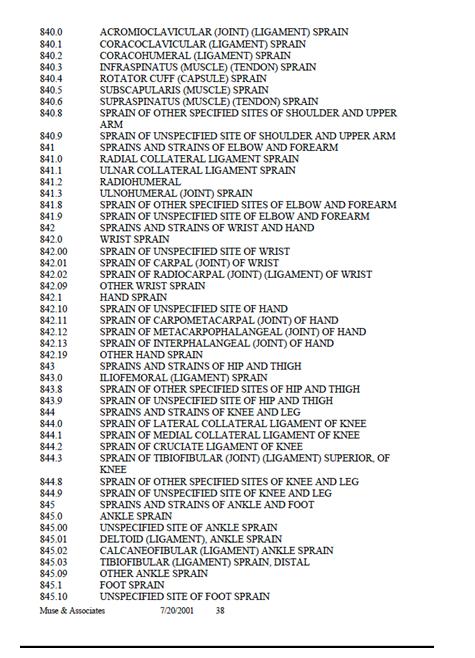
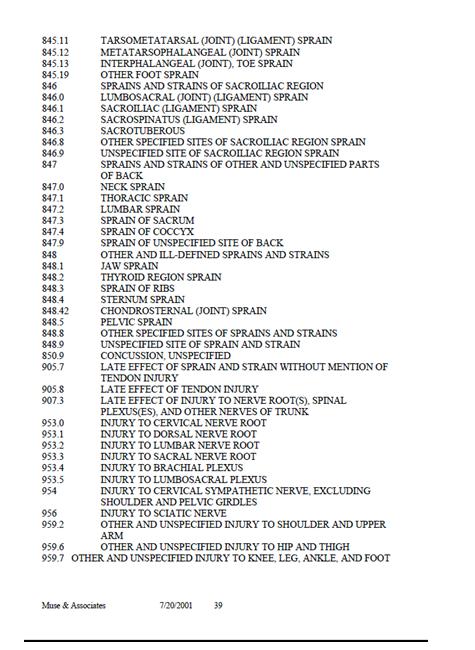
This observation was made because the data used during this study related to conditions that extended to a broad range of ‘Medicare beneficiaries with primary diagnosis of selected musculoskeletal and related medical conditions.’ The common categories found in the study are ICD-9 diagnostic codes 720.xx, 721.xx, 722.xx, 723.xx, 724.xx, 739.xx, 839.xx, 846.xx, and 847.xx. [12]
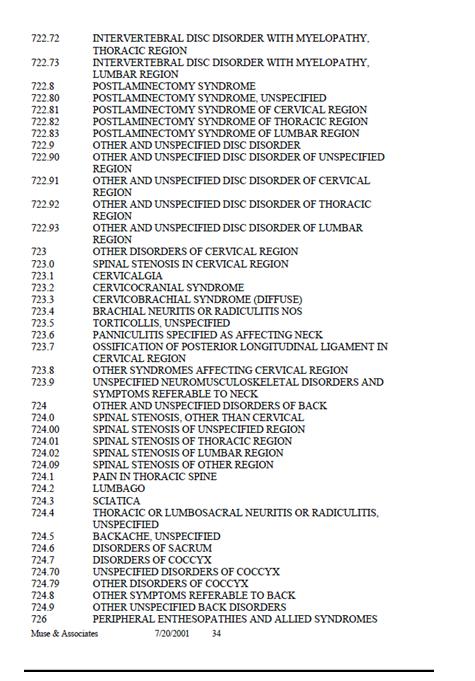
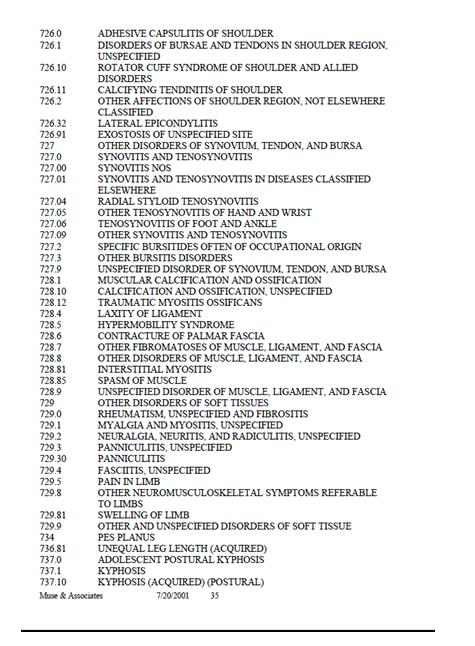
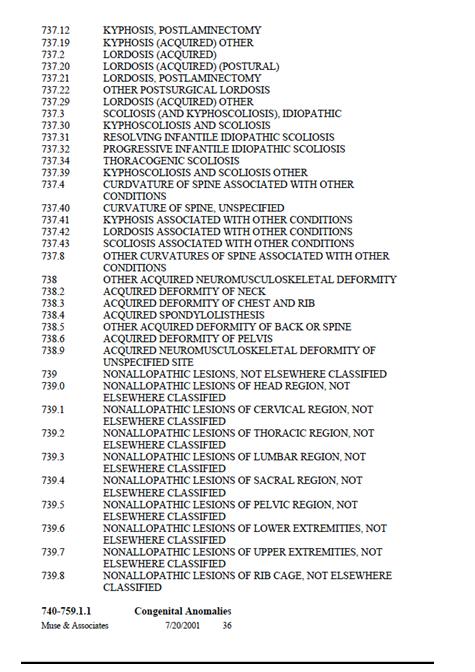
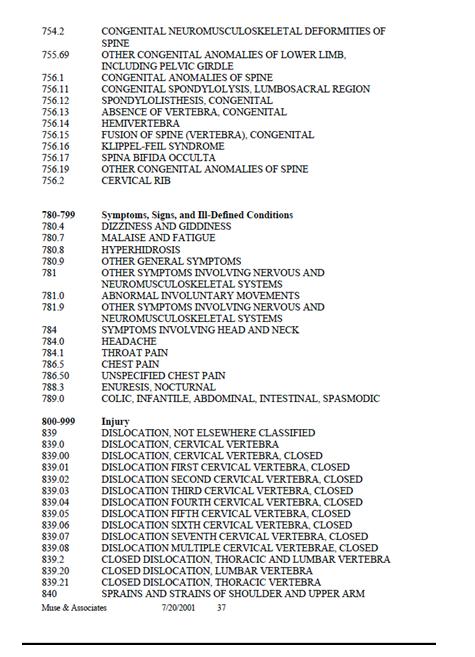
Appendix A, which is listed in this study showed the diagnoses commonly treated by Doctors of Chiropractic, and which was germane to this study, is reproduced below: [12]:
REFERENCES
- World Health Organization. History of the development of the ICD [Online] 2012 [cited 2012 Jul] Available from: URL: http://www.who.int
- World Health Organization International classification of diseases (ICD) [Online] 2010 [cited 2010 Sep] Available from URL: http://www.who.int
- World Health Organisation ICD Version 2010 [Online] 2010 [cited 2010 Sep] Available from: URL: http://apps.who.int
- WHO programmes and projects The WHO family of international classifications [Online] 2010 [cited 2010 Sep] Available from: URL: http://www.who.int
- World Health Organisation Announcement 2010 July 22 [Online] 2010 [cited 2010 Sep] Available from: URL: http://www.who.int
- Amazon.com Coding and Payment Guide for Chiropractic Services: 2010 Edition [Online] 2010 [cited 2010 Sep] Available from : URL : http://www.amazon.com
- Coding Guide for chiropractic services 2008 5th edition [Online] 2010 [cited 2010 Sep] Available from: URL : www.shopingenix.com
- Coding and Payment Guide for Chiropractic Services 2013 [Online] 2012 [cited 2012 Jul] Available from : URL : http://medco.myshopify.com
- Painter F Diagnosis Codes (ICD-9) Commonly Used in the Chiropractic Office [Online] 2012 Apr [cited 2012 Jun] Available from :URL: http://www.chiro.org/LINKS/dx.shtml
- Lyons A L How to correctly assign the diagnosis code for speedy payment [Online] 2010 [cited 2010 Sep] Available from: URL: http://www.docstoc.com
- Manta Find companies connect with customers. About Muse & Associates Inc [Online] 2010 [cited 2010 Sep] Available from: URL : http://www.manta.com
- Muse & Associates. Utilization, Cost, and Effects of Chiropractic Care on Medicare Program Costs July 2001 [Online] 2010 [cited 2010 Sep] Available from: URL: http://www.chiromi.com/